
 By Josh Katzowitz, WCI Content Director
By Josh Katzowitz, WCI Content Director

Two years ago, the average salary for physicians actually dropped. And while doctor incomes have risen the past two years, the increases have been relatively minuscule. According to the latest survey numbers, the average rise in salaries for 2024 was some of the lowest in 14 years, and the majority of physicians still believe they're not being paid enough for how much and how hard they work.
According to the newly released 2025 Medscape Physician Compensation Report, US physician's total compensation rose about an average of 3.6% in 2024, a much better number than the 2.4% drop that occurred in 2022. Primary care physicians' compensation rose 1.4%, according to the Medscape survey (which took information from more than 7,000 doctors), while those in the 29+ specialties that were analyzed rose 1%. Overall, all physicians who were surveyed averaged a compensation of $376,000 – a 3.6% percent increase from the $363,000 they earned the year before.
The 2024 Doximity Physician Compensation Report showed that physicians had increased their pay by 6% in 2023 after a decline of 2.4% the year before. Still, Domixity said that, when adjusted for inflation, Medicare physician payment had decreased by 26% since 2001.
Wrote Doximity:
“While [the 2024] increase appears to be a step in the right direction, inflationary pressures continue to impact physicians’ real income.”
In 2022, physician income and a doctor's purchasing power were hurt by inflation that reached a high of 9.1% that summer. That meant a doctor's net worth also probably decreased, particularly since stocks and bonds both had terrible years in 2022. But inflation stabilized in 2023, and the S&P 500 posted a 24% gain. The S&P posted another 23% gain in 2024.
According to the MGMA 2024 Provider Compensation Data Report, primary care physician and surgical specialist physician total compensation both increased about 4.4% from 2022 to 2023. But nonsurgical specialist physical total compensation only rose 1.81% in the same time frame.
The physicians who were surveyed by Medscape in the 2025 survey weren't necessarily thrilled by their salaries.
Medscape reported that 62% of those surveyed believe that most physicians are underpaid, while 33% believe they're paid just right. The other 5% think most physicians are paid too much. To compare those numbers with Americans who were surveyed in 2021, only 11% thought doctors were underpaid. When the Medscape survey-takers were asked if they thought they themselves were underpaid, only 53% said yes.
As one survey-taker said in the 2024 survey:
“Do I feel I am paid well? Yes, in comparison to other Americans. However, I gave the time, money, and sacrifice to do it.”
In a Doximity article released in August 2022, a survey of more than 1,000 doctors found that 55% of them are either delaying retirement (about 40% of those who were surveyed) or reducing their expenses (about 15%) because of the economic environment at the time. According to Doximity, “Older physicians, who are closer to the traditional retirement age, are much more likely to delay retirement than younger physicians. But a substantial percentage of those in their 30s and 40s are also planning to delay retirement.”
According to Doximity’s latest data, which was gathered with the help of 33,000 US physicians, the gender pay gap slightly narrowed to 23% in 2023 (down from 26% in 2022 and from 28% in 2021), as male doctors earn about $102,000 more than their female colleagues per year (it was a $110,000 difference in 2022 and a $122,000 difference in 2021). That disparity also could have led to more cases of physician burnout.

“While there appears to be slight movement in the right direction, physician pay parity continues to be a critical area in need of improvement,” Doximity wrote. “This pay gap may be contributing to an even higher burnout rate among women physicians, with nearly 92% of women physicians surveyed reporting overwork, compared to 83% of men.”
Doximity also wants to make sure awareness of the issue is being raised.
“One of the most critical steps to closing the physician gender pay gap is raising awareness of its existence,” Doximity wrote. “In a survey of over 1,000 physicians, conducted in February and March 2024, about half (nearly 52%) said they believe there is a disparity in how men and women physicians are compensated. However, gender appears to impact this belief. While nearly 75% of women physicians surveyed believe there is a pay disparity, fewer than 30% of men physicians also believe this is true.”
The latest Medscape data shows the pay gap has widened slightly, as male doctors averaged $415,000 and female doctors averaged $317,000, a $98,000 difference. In the previous year's survey, male doctors averaged $400,000 and female doctors averaged $310,000, a $90,000 difference.
Still, doctors are paid more than just about anybody else in the US. As reported by USA Today in late 2024, of the 20 US jobs with the highest average pay, 16 of those are filled by physicians (dentists and dental specialists make up the other four spots).
Average Doctor Salary
In reality, the average doctor's salary of $376,000 isn't all that useful to know.
As an example: according to the latest Doximity report, the average pediatric endocronologist makes $217,875 per year. The average neurosurgeon makes $763,908. That's a difference of more than $546,000. Which, when comparing those two specialties, means absolutely nothing. Plus, consider that, according to the 2025 Medscape survey, the average primary care physician makes $281,000 vs. a specialist who makes $398,000. That's also a pretty big difference. Here's a quick look at general compensation from Medscape's most recent survey in 2024.
Medscape Physician Compensation Report 2025

It's almost certainly more useful to know the average in a doctor's specialty as opposed to the salary of a physician in general.
Intraspecialty Pay vs. Interspecialty Pay
As Dr. Jim Dahle has repeatedly pointed out, “One of the things I have noticed that no one ever seems to talk about is that intraspecialty pay variation is higher than interspecialty pay variation.”
As Jim noted in a previous post, here’s a chart from 2015 that shows the results of an emergency medicine salary survey. The salaries might be outdated, but the general point remains.

He wrote:
“Look at the 10th percentile for employees—$213,000. Now, look at the 90th percentile for partners—$510,000. Difference? $297,000. GREATER than the difference between the average pediatrician and the average plastic surgeon!
The ability to increase pay and increase it substantially solves a ton of financial problems that real doctors run into and email me about all the time. It's way easier to pay off your student loans or mortgage on twice the income. Even after-tax, it's much easier to become financially independent or have a dignified retirement or send your kids to the college of their choice when you can double your income.”
How Much Do Doctors Make an Hour?
Physician income information is relatively easy to find, but work hours information is notoriously difficult to find. The only information that combined physician work hours with their income is from a survey in JAMA published in 2003 (which obviously uses even older data).
The below physician salary per hour combines the JAMA data with Medscape’s 2024 survey, and it's adjusted for the decreased work hours in each specialty. This chart (possibly erroneously) assumes that all physicians work 48 weeks a year. Where Medscape didn’t have survey data, other less reliable sources were used. Those figures have an asterisk next to them in the table.

Doctor Salary by Specialty
One interesting thing about salary surveys is that they are garbage in/garbage out. Average specialty pay varies significantly between surveys. Before we focus on the Doximity numbers, which you'll find in the paragraphs below, compare and contrast those numbers with the average annual earnings by specialty from the 2025 Medscape survey.


Medscape says infectious disease doctors make $277,000. Doximity says $314,000. That's nearly a 12% difference. Medscape says orthopedists make $543,000. Doximity says $654,000, 20.4% more. What is a new grad or even an established doc who wants to negotiate a contract supposed to do with that much variation between averages (besides using the Doximity survey when negotiating)? But what if you're a neurosurgeon or CT surgeon, and Medscape doesn't report on your specialty? Or you don't see your specialty listed on Doximity? Are you stuck paying to get MGMA data (or hiring a contract management firm)? Is that data even any better than these surveys?
For even further exploration, here are several individual specialties that Medscape looked at in 2023, how much money those doctors make, and whether they think their income is fair:
- How Much Does a Pediatrician Make?
- How Much Does a Radiologist Make?
- How Much Does an Anesthesiologist Make?
- How Much Do Psychiatrists Make?
- How Much Does a Neurologist Make?
- How Much Does a Cardiologist Make?
- How Much Does a Dermatologist Make?
- How Much Does a Urologist Make?
- How Much Does a Pathologist Make?
- How Much Does a Plastic Surgeon Make?
- How Much Does an Oncologist Make?
- How Much Does a Nephrologist Make?
- How Much Does an OB-GYN Make?
- How Much Does a Rheumatologist Make?
- How Much Does a Family Medicine Doctor Make?
- How Much Does a Pulmonologist Make?
- How Much Does a Physiatrist Make?
- How Much Does a Hospitalist Make?
- How Much Do Orthopedic Doctors Make?
- Doctor vs. Dentist Salary
- Where Do Millennial Doctors Make the Most Money (and How Much Do They Make)?
Highest-Paid Doctors
Now, for the Doximity survey numbers that tell us the highest-paid and the lowest-paid doctors. When it comes to the top-earning specialties, those in surgical and procedural specialties dominated the list, and doctors who earn the least mostly practice in primary care and pediatrics.
So, how much do doctors make? Here’s what Doximity found for 2024.

Lowest-Paid Doctors
And here are the specialties that earn the lowest salaries.
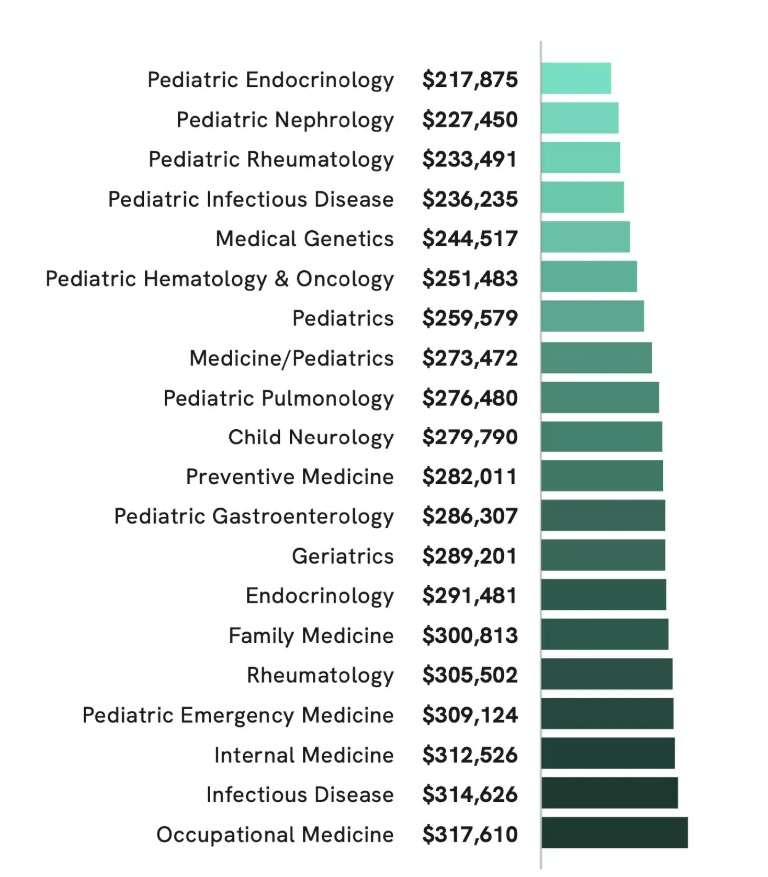
Keep in mind that these charts are of the top-20 highest and lowest average doctor salaries. For specialties like psychiatry, neurology, and geriatrics, those average salaries range from about $289,000 to about $348,000.
As for which specialty's salaries are increasing and decreasing the most, here's a chart put together by Medscape in its 2025 survey.


Doctor Salary by State and Region
One way to get closer to financial independence is to practice geographic arbitrage, where a doctor lives in a lower-cost-of-living area and draws a higher salary where the need for physicians might be greater than those in the big cities on the coasts. The following chart from Medscape in 2023 seems to show that geoarbitrage is not a myth.

Obviously, a doctor living in New York City is going to have a much higher cost of living than a physician who's residing in Weyauwega, Wisconsin. The fact that a doctor in the Badger State probably brings home more money than a physician in the Big Apple is also another point in favor of practicing geographic arbitrage.
In 2025, Medscape released this chart, showing that US doctors make more money in the north central part of the country.

As Medscape notes, “hospitals in rural states with fewer doctors per capita must ramp up their base salary, signing bonus, and loan-repayment options to compete with big-city markets that offer lifestyle advantages.”
Doctor Salaries by Employment Setting
The setting in which a doctor practices also heavily affects how much they earn. As you can see below, via the Doximity survey, the difference between practicing in a single-specialty group vs. working for an urgent care center can be nearly $173,000 a year in 2024.
- Single Specialty Group: $461,000 (a 5.0% increase from last year)
- Multi-Specialty Group: $447,000 (a 6.1% increase from last year)
- Solo Practice: $443,000 (a 3.5% increase from last year)
- Hospital: $428,000 (a 5.8% increase from last year)
- Health System/IDN/ACO: $427,000 (a 7.0% increase from last year)
- Health Maintenance Organization: $406,000 (a 4.9% increase from last year)
- Academic: $365,000 (a 5.2% increase from last year)
- Urgent Care Center/Chain: $288,000 (a 9.1% increase from last year)
- Government: $292,000 (a 8.6% increase from last year)
Need tips for how to increase pay in your specific specialty? Jim has some ideas.
There's plenty more to read in the entire Doximity report—which also includes information on physician compensation in different metro areas, cities with the fastest-growing doctor salaries, and the impact of physician shortages. For comparison, here's Medscape's Physician Compensation 2025 Report.
What do you think? Are you surprised by any of these numbers? Have you found a way to increase your pay inside your specialty?
[This updated post was originally published in 2022.]

I think the most critical piece of information and advice here is how Intra-specialty pay ranges are often much wider than inter-specialty pay ranges. No matter our specialty, there are ways that we can identify, define and solve unique problems that will increase our compensation. We are all also by definition high income earners and can use our doctor pay as seed money for additional often more leveraged income streams!
Intraspecialty pay variation is so true…. People don’t realize this and assume your pay range according to your specialty. I’m internal medicine trained and at the peak of my career I was making 7 figures a year without doing a single procedure.
Tell me more…..
How were you making 7 figures per year?
As a radiologist it’s hard to make that level of income without sacrificing quality
In my experience, rads that make >95th% in income also read >95th% with respect to RVUs (minority will make that type of money owning imaging centers though this is becoming pretty rare), basically no free lunch. Some rads able to do this-seems to be largely related to temperament and the ability to separate oneself from their work to some extent.
Psychiatry has very large intraspecialty differences related to inpatient versus outpatient, group versus solo, employed versus private practice, practice location, call versus not, medical directorship, fellowship status, and many other variables.
I’ve been medical director of something since 1998, taken call throughout, did inpatient on the primary job or as a side gig (since 2011), and these items have pushed up my pay. They come with increased hours, increased work stress, and more weekends and holidays.
My primary job paid $135K in 1994. It took about twenty years to double. Taking on a side gig and working 12-20 “extra weekends” per year and many holidays leveraged the wages up.
Most psychiatrists make $250K to $325K, but as in all other specialties, the hardest working people taking call, doing inpatient work, and working weekends do better. If you are willing to work “harder than the average bear”, one can make $400K to $600K for doing “a job and a half”.
I think this is likely similar in other specialties. Take on a half time side gig, call, and more work…you make more money.
The people who seem to do the best have diversified away from only seeing patients. They own buildings, have NP’s or PA’s working under them, and some “make money while they sleep” with real estate or other endeavors like the WCI.
Couple of thoughts:
1. Lumping a general cardiologist with a procedural cardiologist (or any other lumping of a specialty + procedural version of that specialty) leads to junky data.
2. Lumping a specialty + pediatric version of that specialty together leads to junk data.
3. Lumping VA anything with any other practice setting is junk.
4. Lumping full-time, part-time, and more-than-full-time together leads to junk.
The stats are not usually made by docs, I think, and a lot of important info gets lost. Perhaps it is impossible to do well due to how much variation there is in practice patterns and number of hours worked.
Agree. General surgery is another category with pretty worthless data – it could include so many subspecialties and practice settings that there will be huge variations in compensation.
I don’t think you understand what a general surgeon is
Averages are exactly that…average. Bell curve distributions obviously would be more useful but this gives people a ballpark estimate between specialties. There are companies like Sullivan Cotter which give much more granular percentiles on specialty specific compensation..
How much do they charge for their data?
No idea how much that costs. Our HMO organization uses their benchmarked pay data to adjust our pay.
Great info/discussion. With respect to intra-specialty pay variation, in my field (rads) its essentially a direct correlation with RVU production. Is this different with other specialties?
“Garbage in, garbage out.” This is a great point, and it’s also made worse because it’s sometimes hard as a business owner to know how much you’re making. For a private practitioner (I’m employed), I bet it’s hard to know how much you’re taking home until you file your taxes the next year. You’ve got the practice expenses, the utilities, the various payroll taxes… it goes on and on.
So some of this problem is lack of reporting but some of it could also be that it’s tough to figure out your real salary unless you’re employed and get a paycheck.
Excellent, informative post by Josh Katzowitz. Very useful information. Thanks Dr. Dahle. I enjoy listening to your podcast every week- have learned a lot in the last couple of years about various topics. Not a physician myself- married to one, and also the proud mother of one.
I’m wondering how many doctors here value time more than money, in the sense that we all can make good enough money, and will clearly work long enough to not ever have to worry about it. What’s more, would you sacrifice your health and time with family or doing other things to leave money to family you’ve already taken care of better than 99% of the richest country that ever existed? Some of this stuff borders on bizarre when you … have a few looks at the tax code, and the Jones-ing that most do in society.
Personal time vs money concept is probably why there is a gender gap
NO Probably NOT
On Doximity, they compare compensation. Here, you discuss salaries (until the final graph where you now are showing what is typically compensation breakdowns). I couldn’t find Doximity’s definition of compensation — is it total compensation (ie salary + benefits) or just salary? Important distinction, especially for those working for hospitals or larger groups.
I’m not sure anyone knows, including the folks at Doximity. But you’re right that it makes a difference.
Also, for those doctors that own shares of surgery centers, do these salary numbers include their earnings from these centers? Owning these or not can make a huge difference in your pay & I’d bet for many specialties it separates the bottom 10% from the top 10%.
I agree, but don’t think that’s included in these numbers.
I think these days influencers make more than anyone without any special talents.
Great insight Josh, I’d like to know if these figures are similar or the same to salaries in the UK,?
UK physician salaries are much lower than these figures.
So are Nigerian, Costa Rican, Ukrainian, and Korean doctor salaries. Just like the salaries in those countries for all professions.
The differential I see in physician salaries in the UK compared to other professional salaries in the UK seems much smaller than in the US while in South Korea or even prior Commonwealth countries like Canada and Australia (I don’t have any direct experience with Nigeria, Costa Rica or Ukraine) the physician salaries seem comparatively higher at least from what I see in my industry. It seems unusual because those UK physicians may have roles more significant than my US physicians but their income is substantially lower because salary is set locally.
So do you think UK docs are paid too little or US docs are paid too much?
I am only trying to point out that the gap is large and that UK physician salaries really aren’t similar to this data (maybe around the 10th percentile columns in those compensation tables). I still haven’t met any physicians who think they are paid too much.
Don’t forget it matters here if you’re talking salary or total compensation. I put almost $100k of my salary away for retirement. If you’re a UK doc with a pension you can put away $0 and still be fine. If you really want to compare my salary with a UK doc, you need to drop it by the $100k that goes into retirement to be a fair comparison. Nobody every does that. They just look at the top line number and compare because it’s scarier that way.
Also to WCI’s point, all “average” professionals make less over there. Not just docs
Yes, I am comparing what it costs us as a company to hire a physician in the US vs UK so this is total compensation including any retirement deferments.
This is such interesting information. I was always curious about what doctors made. I have heard the riches are in the niches. It looks like that’s the same for doctors. It is surprising how many hours some of them put in!
Well, my Mom wasn’t wrong when she said “You just have to be a Doctor to save the family) The Pun…
The Reliable Barber shop POS System in the U.K. Our Barber shop POS helps you grow revenue, attract customers, and improve offerings through various modern features.
I just wanted to point out that the difference is huge and UK doctor salaries really don’t look like this data (probably around the 10th percentile on these pay scales). I have yet to meet a single doctor who feels they have been overpaid.
I don’t recall ever meeting anyone who felt overpaid.
But yes, this data is US specific. 99% of our readership is US based. While 95% of our material is applicable to UK docs, this post really isn’t.
I’ll go on the records to state I feel over paid. I’m 5 years out of training and made over $600k last year averaging under 40 hours per week. I will bring up a separate interesting point that pay also changes over your own individual career. For example, my pay was less than half my first year out. So in 4 years I’ve doubled my income. I didn’t change jobs. I just made partner and increased the patients I now see, etc.
You’re a rare bird. I suppose I’m also “overpaid”, but not for my clinical work. Ownership has its privileges. There are risks and hassles for sure, but there’s a reason it’s called capitalism.
What do you do, and are you hiring? 🙂
Didn’t realize this was just a re-post. Surprised to see my old comment on here lol! Update: for 2023 I made over $800k so now my first year out versus 6th year out is 4x difference. I’m an ENT in central texas and yes we are hiring 😉
So your work pays you more because you are working on more patients, are you’re a fast worker? (Just wondering)
The article “How Much Do Doctors Make?” on White Coat Investor provides a comprehensive overview of the average salaries of different types of physicians in the United States. It breaks down the data by specialty and provides helpful context and analysis to help readers understand the factors that influence physician salaries, such as location, experience, and practice setting. The article also highlights some of the non-monetary benefits of being a physician, such as job satisfaction and the ability to make a positive impact on people’s lives. Overall, this is a valuable resource for anyone considering a career in medicine or seeking to better understand physician compensation.
This is a valuable resource for anyone considering a career in medicine or seeking to better understand physician compensation.
I read the whole post…then realized I’d read it before. It’s very informative and interesting. The intra-specialty variation is similar to the variation in any service field with opportunities for leverage. There is a reason plumbers charge more for emergencies and weekends.
Total hours and leverage are big wage determinants. Who wants to work weekends and holidays? Nobody. Better get paid more. Who wants a lot of night call? Nobody. Better get paid for it.
In semi-retirement at age 58, I kept all my leverage: work from home, paid night call, and sone weekend and holiday work. These three pump up my pay per hour for the markedly reduced hours. Sixteen hours per week pays about half of my prior full time wages.
Work from home: no commute. Paid night call pays me whether they call or not and total work per night is about 5 minutes (which makes it worth a LOT per hour as I’m working minutes per night.) Weekend inpatient pays up to triple more per hour.
Unfortunately, insurers do not pay more for weekend or off hours work. One can only profit from this if others in the practice are willing to pay for the luxury of extra time off.
Key part of this is hospital subsidization. Hospital CMS reimbursement has kept up with inflation which is not the case with physicians. If hospitals want to maintain certain services that are in high demand-in part due to labor shortage (eg. IR), they will have to compensate appropriately or go without.
Why are we accepting such low pay reimbursements? Tradespeople get paid well along with other professionals in tech, finance. Why are lobbyists not telling cms and payors to increase Rates or at least keep pace with Cola?
If I get called in after hours no extra pay but your plumber will charge extra and we pay it!
That is THE question. The answer is pretty simple. Physicians collectively have all the power, but we have none individually. And it’s hard to get physicians to agree on the color of excrement.
Reading the WCI and achieving financial independence is a great start, allowing physicians to make choices that align with their beliefs on this subject. You can refuse to work for a private equity-owned medical entity. You can aggressively negotiate your salary. You can speak openly of your concerns without fear of the repercussions. As WCI wrote elsewhere in the comments, you can automatically reply that you aren’t paid to answer messages. You have power as an individual because of your financial options.
Unfortunately, this doesn’t extend to our entire profession. Hospital systems, PE-backed entities, and insurance companies don’t care about us as individuals. It doesn’t affect them if you quit, opt out, or get fired. You will be replaced by someone who will walk their line. It will take the collective action of physicians to affect change. Until that happens, we will continue to see the slow, steady erosion of physician pay, autonomy, and job-satisfaction.
I love looking at the numbers of pay per specialty and location. All the numbers above are very relevant but I do think the ‘story’ matters, which I believe accounts for the intra-specialty differences. As WCI and others mentioned in some of the above comments if you are making X or Y it may be simply due to higher call volume (1:3 vs 1:10), different acuity, or working more swing or night shifts which may not be reflective in the data….and all these variables are relevant vs ‘average ortho surgeon in Chicago makes Z’ per year. Many different datasets have different definitions for total compensation (including retirement? Student loans?) and benefits may not be factored into average pay going up or down (is vacation increasing or more parental leave policies being implemented?). If you are in Minnesota it may be very different of course from St Clair to Minneapolis the same as it is different from PE to Private Practice to Employed and academics (or pseudo-academics as it may be)
Overall I love reading articles like this and a big ‘thanks’ for sharing….inputting your “story” in for your situation and how you stack up is very relevant.
And that 55 hour week is really low. Consider that every night we have at least 2 more hours of charting to complete our day. And this does not take into account the on call hours !!
I think the breakdown by hourly pay is important, but very hard to find data on. I’m in pediatric ICU and according to this I make more than the average radiologist or adult urologist …. but I’d bet I work a lot more hours to do it (at least for the next few years). It makes the data even less useful if they include part time people in the “average.”
I suspect the gender wage gap also has a lot to do with this (women are smarter than us men and less greedy. More likely to be part time and less likely to do a ton of overtime). I’d really be interested to see what the gender gap is in hourly pay. I suspect one still exists, but I’d bet it’s less dramatic.
Whenever job hunting I don’t look at the top line number, I always look at the hourly pay to get a true comparison.
I bet the pay gap is nearly completely explained by 1- less likely to be partner/equity, 2- more likely to limit hours for family, 3- more likely to have prolonged time out for kids, meaning having and raising kids. I think in general it’s well documented that income is correlated with number of years continuous employment. Taking a year or two or three to raise kids from an economic perspective would be expected to be devastating to career income in any job.